The Global Coalition for WHO Action on Firearm Violence (GC-WHOA) invites health professionals, researchers, survivor-led organisations, civil-society groups, and government partners to join us in strengthening the World Health Organization’s leadership and accountability on firearm-violence prevention and care.
Together, we can help ensure that the WHO and its 192 Member States act with the same resolve on firearm violence that they have shown on tobacco, road safety, and violence against women and children.
This document outlines the pathway through which a proposed resolution passes within the World Health Organization (WHO) governance system before adoption at the World Health Assembly (WHA). It describes each phase, the key actors involved, and the departments supporting the process. An infographic is also provided for clarity.
Only WHO Member States can formally propose a resolution, though WHO departments, researchers, and civil society partners may informally support the process. Advocates must secure co-sponsorship across multiple regions. The proposal is typically developed with technical input from WHO departments such as the Department for Social Determinants of Health, the Violence Prevention Unit (within the Department for the Social Determinants of Health), and the Governance and Multilateral Affairs Division. Civil society organisations can engage through WHO’s Civil Society Commission, regional offices, and permanent missions in Geneva.
Each of the six WHO Regional Committees reviews draft resolutions. These committees — for Africa (AFRO), the Americas (PAHO/AMRO), South-East Asia (SEARO), Europe (EURO), Eastern Mediterranean (EMRO), and Western Pacific (WPRO) — may endorse, amend, or defer proposed texts. Regional endorsement builds cross-regional legitimacy and increases the likelihood of advancement to the Executive Board stage.
The 34-member Executive Board (EB) reviews and approves items to be included in the WHA agenda. The EB session held in January each year is decisive. The EB examines draft resolutions for technical soundness, financial implications, and consistency with WHO’s General Programme of Work (GPW). An October preparatory session may preview proposals. The Secretariat supporting this process is the Department of Governing Bodies (GBS) within WHO’s Governance and Multilateral Affairs Division.
After Executive Board endorsement, Member States engage in informal consultations facilitated by WHO’s Legal Office and the sponsoring missions in Geneva. Negotiations address operative paragraphs, financial commitments, and linkages to existing resolutions. Drafts are refined in ‘informal informals’ and prepared for submission to the WHA Committee A.
The WHA convenes annually in May. The resolution is introduced in Committee A (responsible for programme and policy matters), debated, amended, and adopted—usually by consensus. If consensus cannot be achieved, the WHA may vote, though this is rare. Once adopted, it becomes a formal expression of the Assembly’s will.
Following adoption, the WHO Secretariat integrates the resolution’s mandates into its Programme Budget and issues a Director-General’s report to track progress. Relevant departments lead implementation, with oversight by the Executive Board. Follow-up reports are typically presented two to three years later.
Implementation involves coordination between WHO headquarters, regional offices, and Member States. Civil society organisations continue to play a monitoring role, ensuring accountability for the resolution’s commitments.
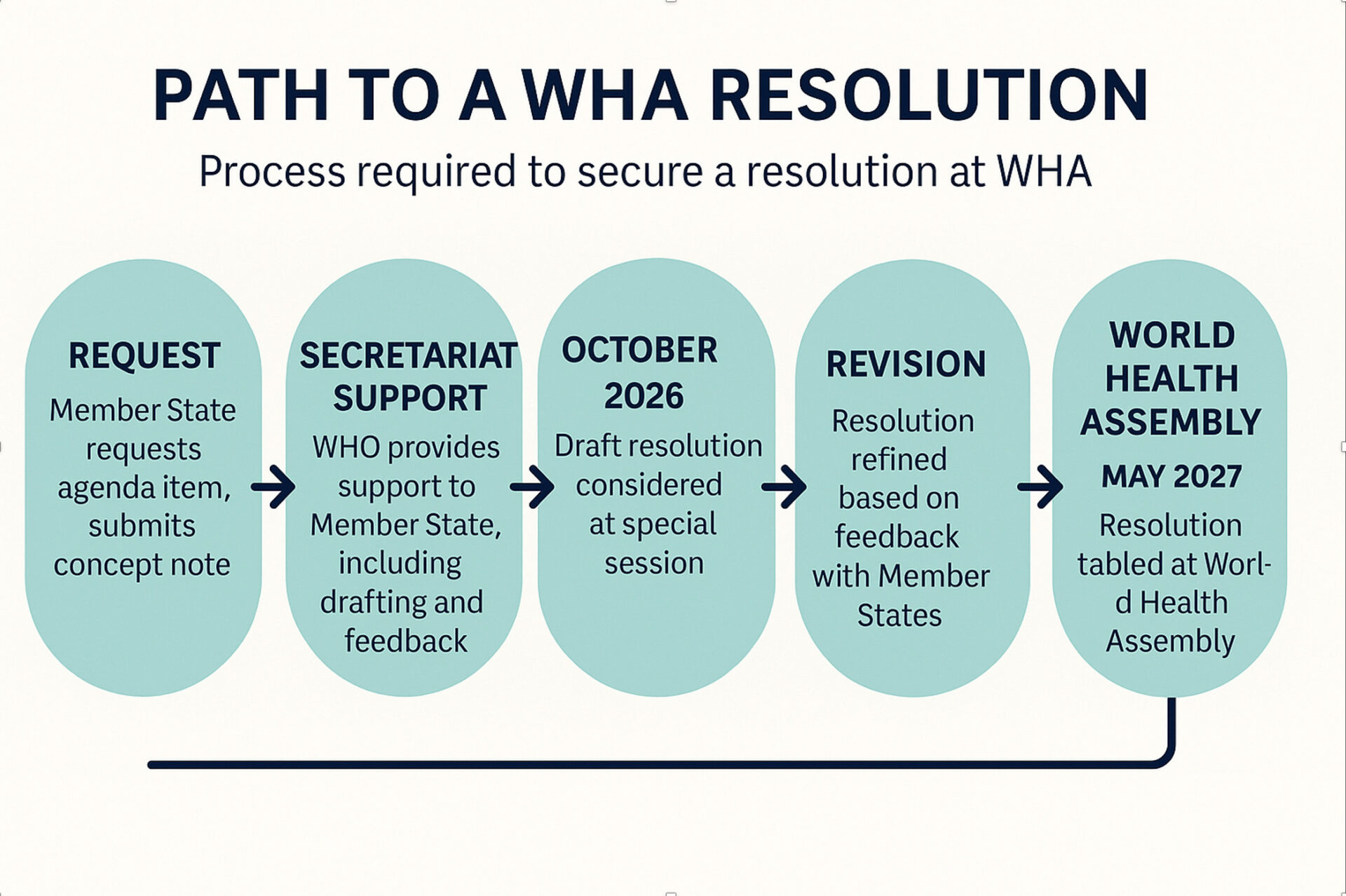
The table below visualises the expected timeline for advancing a WHA resolution on gun violence.
WHO Departments typically involved at each stage include:
| Period | Stage | Key Actors |
|---|---|---|
| Mar–Aug 2026 | Draft concept and secure sponsors | Health ministries, WHO Violence Unit, civil society |
| Aug–Oct 2026 | Regional Committee endorsements | Regional Committees and Member States |
| Oct 2026 | Executive Board preparatory session | EB members, Secretariat |
| Jan 2027 | Executive Board approval | Executive Board (34 States) |
| Feb–Apr 2027 | Informal negotiations and revision | Sponsoring missions, WHO Legal Office |
| May 2027 | World Health Assembly adoption | All 194 Member States |
| 2026–2028 | Implementation and follow-up reports | WHO Secretariat, Member States, civil society |
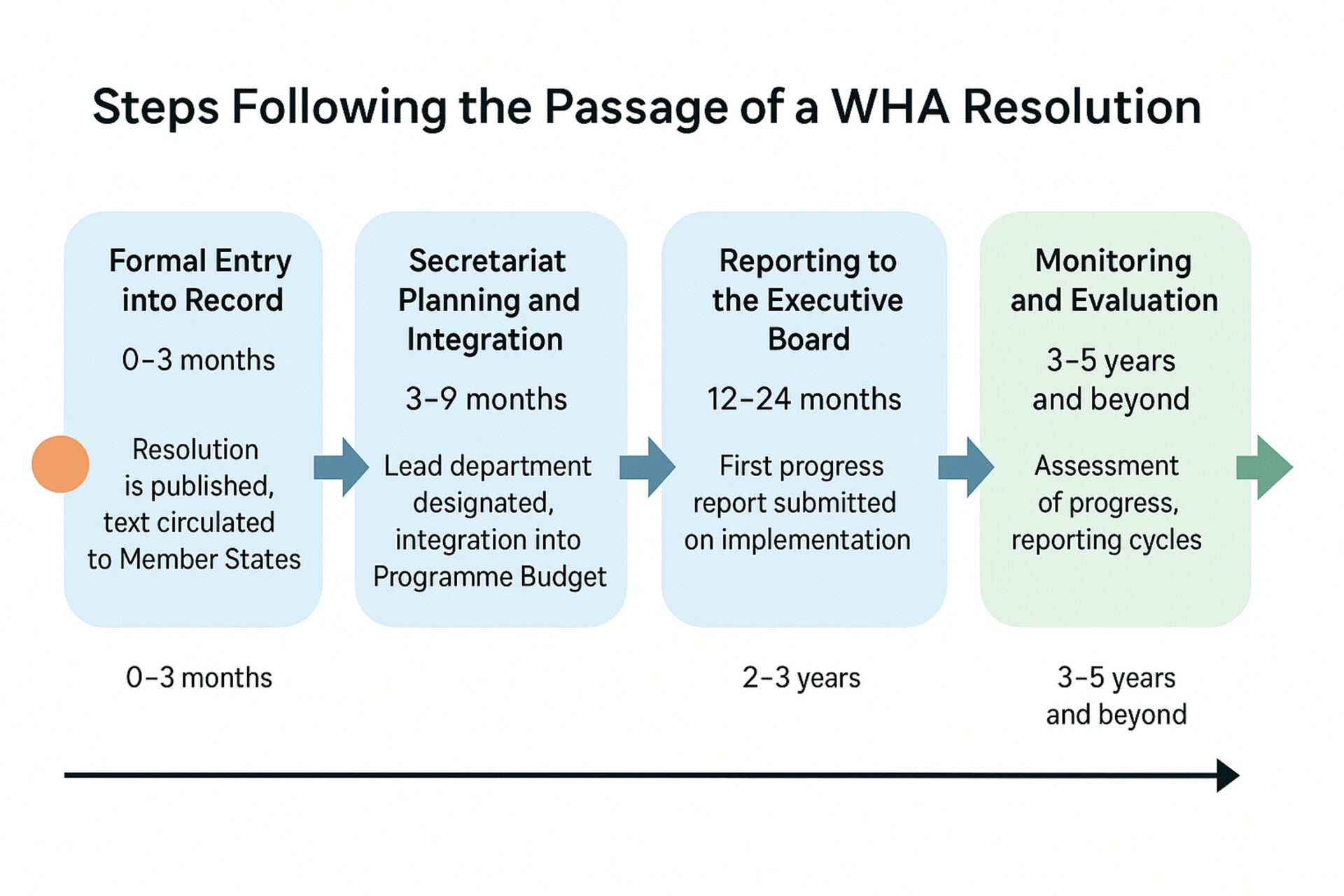
This document provides an overview of the mandatory steps taken by the World Health Organization (WHO) following the adoption of a World Health Assembly (WHA) resolution. It also includes evidence on the impact of past WHA resolutions and two infographics illustrating the process and timeline for post-passage actions.
0–3 months-Formal Entry into Record: After adoption, the resolution is assigned a WHA number and entered into the Official Records of WHO. It is published online in all six UN languages and circulated to all Member States, regional offices, and relevant WHO departments. The Governing Bodies Secretariat (GBS) issues notifications, often accompanied by a Director-General circular.
3–9 months: Secretariat Planning and Integration: The Director-General assigns a lead technical department, which drafts an implementation plan or framework for action. The Programme, Budget and Administration Committee (PBAC) reviews financial implications, and integration into the Programme Budget follows.
12–24 months: First Report to Executive Board: The Director-General submits a report on progress in implementing the resolution, usually within 12–24 months, under the EB’s regular agenda. The report details actions, outputs, and funding status.
24–36 months: Follow-up Reporting to WHA: A consolidated report is presented to the WHA, summarising implementation progress across regions and proposing next steps. This may include new strategies or indicators for Member State reporting.
3–5 years: Evaluation and Impact Review: WHO may establish global mechanisms or indicators to track ongoing implementation, with results reported every 2–4 years.
Several independent analyses and WHO evaluations show that WHA resolutions can produce measurable outcomes, particularly when paired with implementation plans and funding. Examples include:
While resolutions are non-binding, their influence depends on political will, funding, and institutional capacity. Impact tends to be highest when accompanied by defined budgets, follow-up reporting, and integration into WHO’s General Programme of Work (GPW).